Main Content
High Court Ruling Exposes TAC!
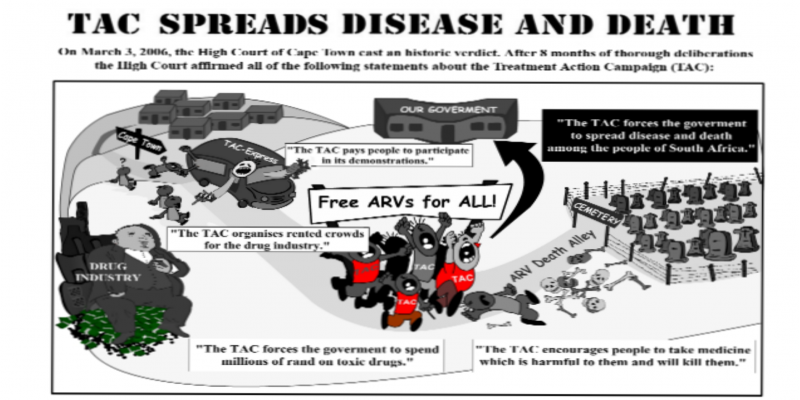
Community News from the Dr. Rath Health Foundation High Court Ruling Exposes TAC! Judges affirm: “TAC forces the government to spread disease and death among the people of South Africa! “ In an historic verdict the High Court of Cape Town exposed on March 3, 2006, one of the most appalling, unethical and inhumane activities in South Africa since the end of Apartheid. The demo- cratically elected government of South Africa is being forced by pressure groups – largely financed by foreign money – to distribute toxic ARV drugs to millions of AIDS patients. The ARV pushing pressure group named in the verdict of the High Court is the Treatment Action Campaign (TAC). BACKGROUND TO THIS HISTORIC VERDICT Masked as a ‘humanitarian’ organization pretending to help AIDS patients, the TAC has been pushing the rollout of highly toxic ARV drugs for years and has been forcing the South African government to spread disease and death among the people of South Africa. Over the past …

No Censorship of Life-Saving Natural Health Information
The people of South Africa now have the historic opportunity to liberate themselves from the yoke of HIV/AIDS and many other diseases. The solution to these health epidemics does not come from high-priced and toxic pharmaceutical drugs but from public education about the dramatic health benefits of vitamins and other natural therapies. In a series of official recommendations UNICEF, WHO and other United Nations Organizations have encouraged people and their governments – especially in developing countries such as South Africa – to help spread knowledge about the health value of vitamins and nutritional medicine. The dissemination of this information will save the lives of millions of people in South Africa, especially in the battle against HIV/AIDS and other infectious diseases caused by immune deficiencies. But we all must fight for this health freedom. Its biggest enemy is the pharmaceutical business with patented drugs – such as ARVs. This industry promotes diseases as …

Benefits & The Advantages of Using Vegan Protein Powders
Protein is the most important nutrient for the development and health of your body. It is the fuel that gives your body the energy it needs to perform at your best and stay healthy. Unfortunately, most people do not get enough protein. Even more interesting is that even the highest protein requirement will only take you through 80% of your daily protein requirements.
There are some great vegan protein powders out there that are a healthy and convenient option. You should be sure to try a couple and see which one works best for you. However, if you don’t have time to do all the research yourself, don’t worry. There are many guides and research available such as this one: https://www.shapebright.com/best-vegan-protein-powders-review/ or this one here that provides easy access to all of the information you will need to make an informed decision.
How protein is broken down depends on what type of protein you are consuming. Animal protein is broken down more easily than plant protein. This is where you can make a difference. If you are following a plant-based diet then you have the ability to compensate for the protein you are missing out on with the right type of plant-based protein powders.
When you go vegan it is easy to give up things like eggs, milk, and cheese. However, there are lots of protein sources you can use, such as beans, nuts, seeds, legumes, tofu, tempeh, and peas. A lot of those foods are known as complete proteins because they contain all nine essential amino acids. However, it’s important to note that plant-based proteins are not digested the same as animal-based protein.
Sites you Can start You Research into Benefits of Vegan Protein
Amazon: There are plenty of options here. You will find more vegan protein powders than you can imagine, and you can find a wide range of different options for a low price.
Comparison sites: You can find everything from bars to powders here. You will find a lot of options for the price you are willing to pay. You can check out Amazon to find some options that are very reasonable, and you can find some great deals on bars and powders.
Substitutions: One of the things you will need to consider with vegan protein powder is that some options are not suitable for vegetarians. Depending on the protein powder you are using, you may need to sub out some of the plant-based protein. You can check with your store if you have any questions. You can use your best judgment when it comes to substituting.
If you want the most health benefits of the plant-based protein powders, you will want to pay attention to the plant-based protein powder you are using. Another important thing to note is that plant-based protein powders are often very expensive. This can cause you to consider protein powder with animal-based protein as well. Unfortunately, while the quality is great for the lower-cost brands, they tend to be just as expensive as a higher-quality plant-based product. This doesn’t mean that you need to shy away from protein powders with animal-based protein, but you should be sure that the money you are spending is making you the healthiest you possible.
Now that you have the benefits of vegan protein powder, you need to make sure that you are getting the right vegan protein powder. As you look for a quality vegan protein powder, you’ll need to know your options. It’s important to know that there are plenty of great vegan protein powders out there. So, as you search for the perfect vegan protein powder for you, keep in mind that there are a lot of brands out there and it can be a bit overwhelming.
The solution is simple: you need to research a little, do some comparing, and then do some shopping. So, just like you did in school, take the time to look at the options you have, and then find a good match. That way you are able to find a vegan protein powder that best fits your needs and budget.

Best Home Gym Equipment for Small Space (2020 Update)
A year ago, I shared with you the top-selling home gym equipment for men and women. It was largely based on three factors: cost, convenience, and durability. This year, the math has changed, and some of the products that held the top spot no longer do, because the cost of some of them has increased.
So what’s changed?
Some of the current bestsellers have their own workout machines. The companies that make these home gym products do so because they have decided that they have a competitive advantage and they don’t want to pass up the opportunity to introduce their machine.
These are usually large companies that can afford to keep up with market trends and introduce new products, while smaller companies that have a competitive advantage don’t need to worry as much about brand new products. There are many guides to help you choose the best equipment for your home or garage gym. You can find many guides online such as this review guide into Force USA G3 model on the Fitgraded website or this guide here on Menshealth.
You also have to keep in mind that some of the top-selling home gym equipment doesn’t include a workout machine.
For example, you can buy a cheap portable hand bike for $80. If you then use it a couple of times, you can probably fix it by sanding it down. However, if you buy an exercise machine, you can use it consistently.
Cost And Convenience Make People Stick To Their Workouts
 If you can’t afford an $80 portable hand bike, what can you do? You might resort to the treadmill or the elliptical. These are great, but the problem is that there are times when you don’t want to sit in front of a machine in your apartment.
If you can’t afford an $80 portable hand bike, what can you do? You might resort to the treadmill or the elliptical. These are great, but the problem is that there are times when you don’t want to sit in front of a machine in your apartment.
If you have a small house, these are great to use because you can use them for long periods of time without interruption. If you have a large house, you’re still limited to 30 minutes or so at a time. However, if you want to get into shape, 30 minutes is more than enough.
Another advantage of working out at home is convenience. You don’t have to take time off of work or leave the house to get a good workout. There’s also no one counting your reps or watching you. It’s just you and your workout.
Longevity is important, and you should be looking for equipment that will last you a while. This is usually one of the reasons that gym equipment sells well. If you buy a good home gym, you don’t have to replace it every few years. Even if you do need to replace it, the costs are not nearly as bad as if you buy new equipment each time.
Durability Is a Must For All Exercise Equipment
If you’re going to be using exercise equipment regularly, durability is a big deal. If it breaks, you’re going to be in a lot of trouble. The more durable the equipment is, the more likely it is that you’ll keep it up. The upside is that if you get a good deal on a piece of equipment, you don’t have to replace it as often.
Having a workout space at home is critical to building a healthy lifestyle, but if you have a small space, then you might not be able to do it at all.
There are two ways to go. One is a full home gym and the other is just making the most of what you have.
You could do a full home gym, but you would be wasting a lot of space. You also would have to pack it up to move somewhere when you decide to move.
Alternatively, you can split up your home workout space with equipment that can be used in a number of different ways. The best home gym equipment for small space is a multifunctional piece of equipment that you can use in a number of ways, such as squat racks, barbells, or medicine balls.
What to Buy for a Compact Home Gym
Once you decide what pieces of equipment you need, it’s important to find the best home gym equipment for a smaller space. That being said, the best equipment for small space does not need to be expensive. It just needs to work well.
There are a number of good options at your local sporting goods store, like The Home Depot and Dick’s Sporting Goods. For example, these are some of the best pieces of home gym equipment for small space:
Stationary bikes – Space saver exercise machine
It’s easy to get bored riding on the same stationary bike all the time.
It’s easy to get bored riding on the same stationary bike all the time. Dumbbells: For this project, you will need to buy a few dumbbells. You can get them in sets of 8 for about $15-18 each.
For this project, you will need to buy a few dumbbells. You can get them in sets of 8 for about $15-18 each.
Weight bench – Good apartment-sized exercise equipment
This is a piece of equipment that you can also find at a sporting goods store. You could also get it in wood. This is equipment that you can also find at a sporting goods store. You could also get it in wood.
Strength rack -good space saving gym equipment
For this project, you will need a strength rack. You can find them at your local home goods store. This is equipment that you can also find at a sporting goods store. You could also get it in wood.
If you have other pieces of equipment that would be great for your home gym, then you can get them at a home goods store or online

Medicines Control Council Threatens Lawsuit to Health Foundation (published in Ann Arbor Newspaper)
Both the newspaper and the foundation were unimpressed by the MCC’s lawyers’ attempt to silence us. The Mail & Guardian again published the complete uncensored text of our call for free access to natural and traditional health therapies in South Africa in this week’s edition, and it was followed shortly afterwards by the Sowetan, City Press, and Ilanga.
The background to our signature campaign is an unprecedented attack by the MCC on natural health therapies and traditional medicines in South Africa. The motivation behind this attempt to outlaw natural health is the trillion-dollar pharmaceutical investment business’s attempt to eliminate all competition posed to its market by safe, effective and affordable natural therapies.
The bogus justification advanced by the MCC for this proposed legislation is consumer safety. But the fallacy of this is revealed by the fact that while no one has ever died from safe natural therapies, the deadly side effects of pharmaceutical drugs kill more than a million people every year.
Any litigation brought against us by the MCC in an attempt to block the truth will backfire. At trial, the MCC will finally have to disclose its secret membership lists and the identities of all its ‘external experts … from … medical and pharmacy schools’ (per MCC website), who make its decisions. They will be cross-examined in open court on their past and present financial ties to the pharmaceutical cartel – the scandalous rule rather than the exception worldwide.
As the deadly side effects of Vioxx and other pharmaceutical drugs come to light, more and more people are seeking answers in effective and affordable natural health therapies. The MCC’s attempt to outlaw natural health in South Africa on behalf of the pharmaceutical cartel is a last desperate bid to shore up the cartel’s collapsing monopoly on world health based on patented synthetic dugs. This attempt and threaen health of many businesses all over the world.
The MCC is the pharmaceutical cartel’s Trojan Horse within the South African health service. Whereas the South African government has advocated natural health in its national health policies and at the international level within Codex Alimentarius – where it has taken the lead in promoting natural therapies rather than restricting them – the MCC is currently seeking to ban public access to life-saving natural therapies, in conflict with the government’s position.
The Dr. Rath Health Foundation Africa fully supports the South African government.
The people of South Africa will not tolerate the MCC’s attack on their right to natural health and its attempt to sabotage their government’s enlightened position on natural therapies.

Benefits of Eating Apples: Cardiovascular Disease Prevention
“An apple a day keeps the doctor away” may not sound like the most credible medical advice, but a recent study out of the UK found that the old adage may have some merit; there really are health benefits of apples.
In a study published in the British Medical Journal, researchers from the University of Oxford discovered that prescribing an apple a day to people 50 and older could prevent up to 8,500 deaths from cardiovascular disease — including heart attack and stroke — each year.
Researchers say that apple-eating had a similar effect on reducing heart disease risk as daily statin treatment, but with fewer side effects. According to the Mayo Clinic, long-term statin use can lead to muscle pain, liver damage, digestive problems, and increased blood sugar – which can in turn increase risk for developing type 2 diabetes. The team of researchers concluded that small dietary changes, like eating more fruit, can help to delay or reduce mortality from heart disease.
Myriad health benefits of apples
Improving your heart health is just one way that the humble apple can help you stay well. Apples provide a powerful punch of nutrition in a small, healthy package.
A medium-sized apple counts as one cup of fruit — half of the daily amount of fruit that adults need in a 2,000-calorie diet. Apples are also a good source of vitamin C, providing 14 percent of the total recommended daily value. What’s more, apples are among the few foods you can eat more of to lose weight — they’re a sweet, satisfying snack that delivers less than 100 calories per serving.
Apples also contain quercetin, a type of flavonoid (a group of plant pigments that give fruits, vegetables, and flowers their color).
Flavonoids are powerful antioxidants, and quercetin has both anti-histamine and anti-inflammatory properties. According to the University of Maryland Medical Center, quercetin may help protect against cancer, heart disease, hypertension, and even asthma and allergies.
How to eat more apples
A nutritious snack that improves your nutrition, promotes weight loss, and helps you exercise more efficiently — how can you get more of that? While an apple is easy enough to eat on its own, having a variety of ways to enjoy apples can help you add more of them to your diet.
While you may think of apples as mainly a between-meal food, there are many creative ways to use apples in recipes at every meal. Try these tips and apple-based recipes from Eating Well to expand your repertoire:
- Start your day with apples. While fruit salad is always a winner at breakfast, don’t stop there when it comes to eating apples. Get creative with a Triple-Layered Apple Breakfast Sandwich. If you prefer something even more luxurious, try this Baked Apple-Cinnamon French Toast recipe.
- Add apples for lunch. For midday fare, try Roasted Pumpkin-Apple Soup. The recipe makes about 12 one-cup servings, so you’ll have plenty of leftovers. The soup contains four large apples of the Empire, Braeburn, or Cameo variety. Add a Curried Scallion Appled Salad for a complete meal featuring your favorite fall fruit.
- Dinnertime apples. There’s no shortage of amazing dinner recipes that give apples a starring role. For starters, try Chicken and Spiced Apples for a savory-sweet meal. Apple-and-Fennel Roasted Pork Tenderloin is another delicious option.
- Twists on apple desserts. While old-fashioned apple pie is always a crowd-pleaser, you can up the ante after dinner with some new taste sensations. If you’re feeling festive, try Apple Cupcakes with Cinnamon-Marshmallow Frosting. For something simpler but still a hit with all ages, bake some Apple-Cinnamon Fruit Bars.
Whether your goal is to decrease your risk of chronic diseases, get more antioxidants, lose weight, lower your cholesterol or glucose levels, get more vitamin C, or simply try some new recipes, apples are the way to go. This all-around fruit is good for what ails you — and all it takes is eating one a day.

Top Massage Chair Brands: [Health Trends for 2019 & Beyond]
If you’re thinking of buying a zero gravity massage chair there are a dizzying selection of options available. Indeed, if truth be told, the vast majority of top-end and midsize massage chairs provide a zero gravity seating position; really for anybody willing to spend more than a couple of thousand dollars it can be more difficult to find a massage chair that is not zero gravity.
The purpose of this article is so simple; to help you limit your options to just the very best zero gravity massage chairs on the market.
While each massage chair owner will have their own opinions about what is”best” we’ve tried to remain unbiased in this article. The top recommendations here are based on the quality of the massage supplied, our own experience with a range of popular massage chairs and feedback from website visitors.
Indeed, in order to help us create this article as valuable as possible, if you have experience with any of the massage chairs listed here, or you still have questions at the end of the guide we would encourage you to use the comments section at the end to get in contact.
Best Massage Chair Reviews 2019
 Here is overview of the top massage chair models in the industry as of [Summer 2018]. I come across more detailed massage chair reviews elsewhere, but this is just an overview of what industry think is the best.
Here is overview of the top massage chair models in the industry as of [Summer 2018]. I come across more detailed massage chair reviews elsewhere, but this is just an overview of what industry think is the best.
#1: Inada Sogno Dreamwave Massage Chair
Inada is the”first” massage chair manufacturer, and their Dreamwave model is thought to be the best massage chair on the market.
It provides more features and a better massage experience than arguably any other zero gravity massage chair on the market — though at a price. Those willing to stump up the princely sum will discover an unrivalled 100 massaging airbags beneath the surface, 16 preset programs ready to knead away tension and pain and built-in heating to further add to the overall experience.
#2: Osaki OS-7200H Massage Chair
Just pipped to the post of the best zero gravity massage chair is the OS-7200. This executive-grade massage chair is also not cheap — but as with all these instances when it comes to massage chairs you actually get what you pay for.
With its heated neck massage feature, six different massage styles and 8 preset programs that this full-body massage chair promises to reach the areas that other chairs cannot — and all while reclined in a full zero gravity position.
#3: Panasonic EP30007 Massage Chair
Arguably Panasonic’s best massage chair, the EP30007 arguably provides more massage choices than any other chair on the market. This includes eight core massage types, five distinct types of massage and a specially designed neck massage designed to feel the same as a masseurs hands.
Bonus: Panasonic EP1285
The truth is that the best zero gravity massage chairs are all have a nifty price tag on.
Therefore as a bonus we wanted to feature a lower-cost option. For those individuals looking to buy a zero gravity massage chair, but reluctant to shell out the big bucks required for one of the seats mentioned previously there *are* a few alternatives.
Of these the Panasonic EP1285 still offers a zero gravity option but in a much more reasonable price. With its different massaging activities and four massage styles it’s little wonder that this impressive chair is currently the only massage chair on the market to be approved by the American Chiropractic Association for its realism and health-boosting advantages.
What’s a Zero Gravity Massage Chair?
If you’re new to the fantastic world of massage chairs the very concept of”zero gravity” may not be clear. Before we jump to our top three zero gravity massage seats it may be beneficial to rapidly define the”zero gravity” principle.
In essence massage seats that offer a zero gravity alternative aim to replicate the posture which astronauts are put into when going into space. This is a position which has been shown to minimize pressure on the joints; particularly important for astronauts being taken into space at several hundred miles an hour.
However the same principle applies just as well to massage chairs. The zero gravity position can help to instantly relieve tension and reduce pressure on the back, neck, shoulders and so on. Massage chairs offering this attribute can therefore offer not only greater comfort but also pain-relieving advantages.
So what exactly does the zero gravity posture look like? In essence the chair reclines to approximately 170′, while the leg rest rises up. The last position is not one where you lie completely flat — that can place pressure on the spine. Instead the body is softly and naturally bent, with the knees positioned over the hips.
Most massage chair users discover that while the idea seems strange, zero gravity massage chairs really do offer a significantly more enjoyable (and beneficial) massage experience than those without this attribute.
Right, so with that from the way the question is really what the best zero gravity massage chair really is? Keep reading to discover our top three picks which are worthy of your consideration…
So, What is the best Massage Chair?
Truth be told, we have not tested out and compared every single massage chair on the market. But from the dozens we *have* tried we feel that the Inada Sogno Dreamwave provides the ultimate in home massage luxury. Having said that, the Osaki 7200 does come a very close second, and is slightly more reasonably priced.
For a lower-priced option we’d encourage you to check out the Panasonic EP1285 for it’s impressive range of features.
In closing the following comparison chart provides basic information on each chair allowing you to make fairer”like for like” comparisons between the different options on the market.